6
Draining and Constraining Agency
I: Changing Habits
Although physicians can fool themselves – and they do so surprisingly often – the sales reps who visit their offices are pretty transparently engaged in sales. Tactics vary widely, and some don’t look much like high-pressure selling, such as the precise ‘detailing’ of the drugs in their portfolios, which involves providing key physiological, pharmacological and prescribing information. But in the end the sales reps are clear that they’re sales reps, making them some of the more visible hands of the pharma world, and some of the less ghostly marketers in this book.
In the first half of this chapter I show some of the work sales reps do to try to shape physicians’ actions, making those actions less independent than they appear. Sales reps have a range of tools to influence doctors, meaning that they can respond differently to different doctors and situations, gaining advantage no matter what their target doctors do. Almost invariably, the result is more prescriptions. In the second half of the chapter, I show the work of a specialized follow-up group of invisible hands, experts in increasing patient adherence to doctors’ prescriptions – increasing rates of filled and refilled prescriptions. Like sales reps, patient adherence specialists have a range of tools, and can respond differently to different patients and situations. Both sales reps and adherence specialists, then, can effectively drain and constrain the agency of their targets.
In almost every detailed account of the work of pharmaceutical sales reps, their overarching goal is stated in terms of ‘changing prescribing habits’, or some close variation of that phrase. Sales reps want to increase the number of prescriptions, or ‘scripts’, for their products, ‘changing physicians’ prescribing behaviour’ in favour of those products. In these phrases, we can see a behaviourist model of the physician. At issue are behaviours and habits, not decisions.
Jamie Reidy, the affable author of the book Hard Sell (which led to a loosely inspired movie, Love and Other Drugs), puts this bluntly:
An official job description for a pharmaceutical sales rep would read: Provide health-care professionals with product information, answer their questions on the use of products, and deliver product samples. An unofficial, and more accurate, description would have been: Change the prescribing habits of physicians.1
In sales reps’ accounts of their tactics, the physician is implicitly a creature whose pen is hovering over the prescription pad as they consider the patient in front of them. What will they write when the pen touches the pad? The sales rep’s job is to induce a specific prescription, a specific ‘script’ for the doctor and patient to follow. Michael Oldani, a sales rep turned anthropologist, writes, ‘Once doctors form these habits, it takes either a new and improved class of medications or a lot of resources (expert speakers, money, and more gifts) to change that habit.’2 We’ve already seen the expert speakers, so I’ll turn to the gifts and money.
Gifts and Money
Oldani argues that strategic gift-giving is the most important element of the relationship between sales reps and physicians. There is a long history of anthropological studies of gifts, and from those studies Oldani emphasizes two elements: the ‘spirit’ of the things given, and the importance of a ‘third party’ in the gift-giving. In pharma, I interpret these two elements in terms of relationships and a reference – however subtle – to the care of patients.
Gifts from one person to another almost always either establish or express relationships. Ideally, they are well chosen for the recipient, or communicate something about the giver. This is why cash – the most neutral of goods – is an inappropriate gift in most situations, unless perhaps it is wrapped nicely and comes with a personalized card. Precisely because interpersonal gifts convey relationships, they demand reciprocity. There is a paradox here, because, unlike an economic exchange, a gift appears not to, but in fact does, demand repayment.
When pharma’s sales reps give gifts to physicians and their clinics – the most standard gifts come in the form of free lunches for staff – there is also some gesture toward patient care, or perhaps toward medical education or research that will affect patient care. This lends gifts legitimacy, making them distinct from bribes.
When Oldani was trying to make his quota for an antibiotic in his portfolio, he focused on a hospital and designed a nearly-perfect generic gift: a card worth ten free cups of gourmet coffee from the hospital’s coffee cart, with the antibiotic’s name on the reverse of the card. The cards were quickly in high demand among residents, staff doctors and the hospital pharmacists. Free coffee communicated that Oldani understood the sleep-deprived culture of the hospital, and that he was caring for the people who worked there. ‘[S]ales far exceeded my expectations and I achieved my quota.’3
Kimberly Cheryl is the author of a bitter book, Escape from the Pharma Drug Cartel, about her former life as a sales rep and her eventual sense of betrayal by the industry. For Cheryl, ‘[w]hatever obligation doctors felt to write scripts for my products usually came from the general sense of reciprocity implied by the ritual of gift-giving’.4 This could sometimes get out of hand:
My career as a caterer began. I arranged to buy lunch for the staff of certain private practices every day for a year. I often invited a group of physicians and their guests to high-end restaurants, bought drinks and lavish meals. I scored sports tickets for my favorite physicians.5
She reports that she distributed ‘unrestricted educational grants’, a tool mentioned by another former sales rep.
The highest prescribers receive better presents. Some reps said their 10’s [the very highest prescribers] might receive unrestricted ‘educational’ grants so loosely restricted that they were the equivalent of a cash gift, although I did not personally provide any grants.6
Even research and educational grants that aren’t convertible to cash can easily be gifts, if they are awarded in the right way. At one point my research brought me into contact with a former sales rep (technically a ‘medical science liaison’, but acting as a sales rep) who spent several years working on only a single expensive product, with a beat of slightly more than a dozen specialist physicians. He also had a sizeable budget for research grants, which he used strategically. Every time the prescriptions of one of his physicians fell below the level he wanted to see, he would visit them and offer them a $10,000 or $20,000 unrestricted research grant. Prescriptions would follow.
Small gifts are much more ubiquitous. Two kinds of small gifts stand out: food, and drug samples. The food part is obvious, because food is the most common tool for building relationships in all walks of life. Reidy jokes that ‘the way to a man’s heart may be through his stomach, but the way to a doctor’s heart went straight through his office staff’s collective stomach’.7 Sales reps try to figure out what offices want, and to be just creative enough to stand out from their competitors. Cultivating a rapport with the receptionists and nurses translates into time with physicians. Imagines Reidy: ‘I can hear it now: Ban the pharmaceutical salespeople! Without drug reps, though, who would bring free lunch to the receptionists and nurses every day?’8
Drug samples serve multiple purposes. They are gifts to physicians that can be re-gifted to patients – perhaps saving the patients money and time on the first few doses of a drug. This makes samples exemplary gifts, since they directly contribute to medical care. But they also encourage the physician to start a prescription with the samples at hand, rather than some other drug.9 Cheryl observes:
Sampling may be the single most important factor in a pharmaceutical rep’s success. Once a patient is started on a sample medication and is doing well on it, physicians are usually very reluctant to change. Therefore, it is essential and vital to have a significant and prominent presence in the sample cabinet of a medical office.10
John Virapen, writing about his work as a sales rep travelling from town to town in rural Sweden in the 1980s, tells the story of how he filled his physicians’ cabinets with his samples. At the onset of flu season, he explained to physicians that he wouldn’t be back for a few months. He wasn’t allowed to leave large stocks of samples, but,
‘We can solve that. It’s only in the best interest of your patients. Look here, I’ve brought you a few extra receipts, one for this month – and these are for the next months.’ …
With a shrug, [the doctor] went ahead and signed the predated receipts.11
The result was a cabinet crammed with his company’s drugs, rather than those of the competitors. Oldani, working in a context in which providing samples was more routinized, explains the art:
[T]he actual placement of samples within a ‘sample closet’ could influence prescription-writing practices of doctors. In many cases, you needed to place your samples at ‘eye level’, especially if your product was one of other medications in a similar class of drugs. Reps would engage in ‘sample wars’, that is, moving competitors’ samples to the back of the closet or out of sight in order to have the doctor or nurse focus their gaze only on our product. … A classic technique was to get your samples placed on the doctor’s desk as a reminder of his or her commitment to using (writing for) your product.12
Samples promote specific prescriptions, tell the physician how much the sales rep cares about patients, and are valuable because they can be re-gifted. In the end, however, all gifts are important, if they are the right ones. One website reminds sales reps, ‘Always remember the fastest way to convince any doctors is by giving them gifts according to their personality.’13 Perhaps this is why a 2010 ruling in a discrimination suit against Novartis found that the company expected its female sales representatives to be ‘available and amenable to sexual advances from the doctors they call on’.14
The Playbook
Sales reps typically enter a physician’s office already knowing many things about that physician and their practice. They often have access to prescription records, sold to their companies by firms that collect data from pharmacy chains. They already know which drugs the physician prescribes, and have a good idea of what the practice looks like. As one training guide puts it, an ‘individual market share report for each physician … pinpoints a prescriber’s current habits’.15 Sales reps also enter with playbooks: however their targets act or react, they have ready responses. If the sales reps have enough information, good instincts and detailed enough playbooks, they effectively trap their targets, denying them meaningful agency in the situation.
The playbooks divide physicians into categories, with a variety of ‘profiles’ or ‘personality types’. A humorous article on a website for sales reps lists six personality types of doctors that the reps meet: Techie, Curmudgeon, BFF, Pupil, Super Ego, and Lost Cause.16 To the extent that this list works as humour, it’s because of all the more serious lists based on prescriptions of the drug at issue or tactics for the sales rep to use. Cheryl’s personal playbook was based on the immediate context. ‘If the doctor was busy or was in the middle of a crisis, the smart representative would discreetly leave samples, get the signature and leave. … If their body language indicated that they only had a few seconds, I would go directly into my sixty-second presentation with product, features, benefits and closing.’17
Even when sales reps don’t have formal playbooks, they keep detailed records on their physicians. Writing about Sweden in the 1980s, Virapen explains the practice of profiling that he and his colleagues undertook, which included information about the practices’ patients, and the drugs prescribed. To get that information might have required first developing a relationship, and finding out about a physician’s ‘age, marital status, number of children and all their birthdays. You need good ties to them, the more the better. Which hobbies, favourite cars, favourite wine, favourite music? … You create a psychological profile.’18 Anything can be put to use. Tracy Krane, a novice sales rep at the time, describes a dinner with her director of sales, Alec Burlakoff, and Steven Chun, a potentially very high-prescribing physician for an expensive drug. Krane
marveled at the way [Burlakoff] drew on a wealth of information about the doctor – intelligence gathered over the course of years – without letting on just how much he knew. Before he worked for Insys, Burlakoff worked for Cephalon, Insys’s chief competitor, and he knew a bit about Chun’s romantic history. … He also knew that Chun liked to visit the casinos up in Tampa, so Burlakoff made a point of talking about his own penchant for gambling. … She had no idea if he was telling the truth.19
We can see a tactics-based list in a useful and insightful short article by Adriane Fugh-Berman and Shahram Ahari.20 Fugh-Berman is a physician who studies the industry, and Ahari is a former sales rep who served as an expert witness in a court case in the US. In the case and the article that followed, Ahari provided a rich description of the ordinary tactics that sales reps employ. His short classification of physicians breaks them down into categories: ‘Friendly and outgoing, Aloof and sceptical, Mercenary, High-prescribers, Prefers a competing drug, Acquiescent docs, No-see/No-time, and Thought leaders’. In a clean chart next to each of these categories Ahari provides his approaches and explains how they work. I’ll elaborate on a couple of his categories as examples.
Aloof and Sceptical Physicians
One of Ahari’s categories is the ‘aloof and sceptical’ physician. This is the kind of target who asserts superiority over the sales rep, claiming to prescribe purely on the basis of hard evidence. Dr Krueger, a KOL interviewed for this book, might serve as an example of the aloof physician:
If a drug company tries to promote things that are not correct the doctor is going to figure that out … Well, you know, being a doctor I guess I am a little biased but my thought is that well it’s not like the guy’s gone to medical school for four years, done a residency, and whatever his or her specialty is – they probably have a pretty good insight into what’s true and what isn’t.
Since their prescribing is science-based, sceptical physicians probably see themselves as the least susceptible to sales reps’ influence. In fact, though, pharma has more resources to throw at these prescribers than at any others.
Pharma sales reps distribute the companies’ preferred knowledge directly to physicians, for example by providing reprints of ghost-managed articles. The fact that they provide knowledge actually legitimizes their presence in physician’s offices. Addressing an audience of publication planners at a large conference, Ms Lane, a former sales rep and now a fiery industry consultant, gives a bit of a pep talk about the importance of journal articles: ‘Folks, they’re dying for your work, by the way. Field reps are dying every day for more of your work. You know that, right? Because that’s what doctors are going to see.’
Ultimately, it is the fact that sales reps provide information, whether in the form of scientific reprints or product information sheets, that legitimizes their presence in physicians’ offices. The transmission of medical knowledge is what allows sales reps to make their pitches, offer their friendship, and convince physicians to prescribe specific drugs.
Oldani writes that ‘these tremendous R and D budgets and the entire flow of knowledge and information used to discover new products rests on the ability of the industry to convince those who can write a prescription … to write that script for their particular product’.21 For the sceptical physician, the relationship also runs in another direction. The ‘entire flow of knowledge and information’ is there to be used to convince prescribers ‘to write that script for their particular product’.
Ahari describes how, in dealing with the sceptical physician, he would ‘play dumb and have the doc explain the significance of my article’. Then, the ‘only thing that remains is for me to be just aggressive enough to ask the doc to try my drug in situations that wouldn’t have been considered before, based on the physician’s own explanation’.22 It’s an ingenious move, because the journal article allows the physician to verbally provide the evidence for the new prescriptions. The sales rep only has to ask the physician to try writing prescriptions for the drug in, say, the next five patients who present appropriate symptoms. That may be enough to establish a new prescribing habit.
Though they may sometimes choose to play dumb, sales reps have extensive knowledge about the drugs they’re representing, the competing drugs, and the conditions for which all those drugs might be prescribed. All this information has been drilled into them in training events, and they’ve continued to study it since. Cheryl recalls her initial training session: ‘Training was four weeks of living hell.’
I will never forget days of constant grinders. We stood in two straight lines. One group played that of a physician, one the representative. We finished one detail and rotated our way down the line. We detailed until the corporate message came to us flawlessly. We knew the key messages for each product. We knew the data on the graphs and how to use them to sell and make our drugs look better than our competitors.23
She proudly claims, however,
I can still detail every bit of information of every product I sold, including the drug’s molecular weight. We [could] go toe to toe in any discussion on just about any medical issue with a physician and we weren’t uncomfortable with our knowledge.24
Reidy also reports weeks of learning about the drugs he would promote, their pharmacological properties, and sales pitches. ‘I began dreaming at night about detailing trainers playing the role of doctor. … Again and again, we detailed each other; people rehearsed over lunch, in the hallways, even in the bathrooms.’25 Against this kind of drilled-in expertise, the sceptical doctor will give way. But many doctors, like Dr Koren, are firm in their beliefs about their ability to do their own thinking:
I mean, to me it’s an insult to physicians that we can’t recognize bias and we can’t sift through it. I mean, we’re more trained than any professionals who make life and death decisions so by saying we need to restrict access to information that’s provided by pharmaceutical companies is basically to say that we’re not smart enough to make our own conclusions – but if we are smart enough then it’s an invaluable source of information that many of the companies are paying for.
Friendly and Outgoing
Sales reps establish relationships with all their physician targets, using whatever common interests they can find, and what Ahari calls ‘finely titrated doses of friendship’. Most reps don’t need much training to be friendly. Reidy describes the boot camp he attended to kick off his sales rep job at Pfizer: ‘With few exceptions, every one of my 149 classmates was impossibly friendly. I had never spent time with so many people who were as chatty as me, and it was fairly annoying. When would I get to talk?’26
Ahari recounts: ‘During training, I was told, when you’re out to dinner with a doctor, “The physician is eating with a friend. You are eating with a client.”’ Physicians do sometimes see sales reps as their friends: ‘Sometimes we don’t even talk about drugs, we just chat about the kids and it’s good to have a relaxed and friendly lunch’, explains one physician.27 And they can have good reasons to see their friendships with sales reps as genuine, as Dr King does:
A good number of my very close friends are sales representatives. … I like to think that those are real relationships just because they’re relationships – and even when people have moved on to other companies or don’t sell a product in my disease state. … Like last weekend I had two other couples who are both representatives – neither of them call on me anymore – over for dinner and a swim party.28
Although friendship is a tool across the board, it becomes the overarching tool for those targets who are friendly and outgoing. ‘I frame everything as a gesture of friendship’, explains Ahari.
I give them free samples not because it’s my job, but because I like them so much. I provide office lunches because visiting them is such a pleasant relief from all the other docs. My drugs rarely get mentioned by me during our dinners. … When the time is ripe, I lean on my ‘friendship’ to leverage more patients to my drugs … say, because it’ll help me meet quota or it will impress my manager, or it’s crucial for my career.
These physicians, meanwhile, genuinely appreciate the interactions. One tells a story in which
they stopped allowing reps in my office, and this one had information for me, so I told her she could join me for a run. She went not only the extra mile, but an extra 2 miles and talked to me about the product the whole way. That was really helpful. You bet I still see her any time she wants to see me.29
Again, the ‘friendly and outgoing’ physician who wants to go running or swimming with reps is just one among many. But there are other approaches that work for the ‘Mercenaries’ (trade gifts for prescriptions), ‘High-prescribers’ (establish strong personal connections), ‘Prefers a competing drug’ (wear them down), ‘Acquiescent docs’ (pair commitments with gifts), ‘No-see/no-times’ (focus on the staff), and ‘Thought leaders’ (provide speaking opportunities).
Influence
Most of pharma’s customers want drugs to be part of a rational world centred on health: drug decisions should be based entirely on solid evidence about their health benefits and costs, not on advertising, hearsay, or fashion. Though prescribing habits may be one of the best studied and precisely understood of markets, physicians routinely claim not to be personally influenced by all the things pharma throws at them. Pharma companies are happy to maintain this fiction, as they never want obvious marketing to overshadow science in importance. Sales reps know this. Cheryl describes a subtle dance in which physicians pretend – often to themselves – that they aren’t affected by sales reps’ actions:
When the encounters between a physician and drug rep went well, there was a delicate ritual of pretence and self-deception. I began to pretend that I was still giving the physicians impartial information and the physicians pretended to take me seriously. My job was to influence the physician in any way that I could while the physicians told themselves that they weren’t being influenced.30
The result is changed prescription habits that allow the prescriber to maintain a sense and appearance of integrity. The reps laugh amongst themselves:
The most comical thing is doctors’ attitudes. You will never hear a physician say, ‘This is influencing me.’ They are just so arrogant and naive.31
Not only do physicians tend to believe that they are immune to pharmaceutical company influence, but their confidence about their immunity increases with the amount of contact they have with industry representatives.32 This is a finding that resonates with the theory of cognitive dissonance: the greater the internal conflict, the greater the likelihood and volume of denial.
All of the tools that a playbook might hold are tools of influence, designed to change physicians’ behaviour. In addition, the playbook as a whole works to constrain and drain physicians’ agency. Whichever way physicians turn, however much they feel they are making decisions, sales reps have a response that pushes them in the direction of specific scripts.
II: The Adherence Problem
As we’ve seen, pharma companies invest enormous amounts of money into producing and shaping medical information, transporting that information to physicians, guiding those physicians to act on the information in particular ways, and prodding patients to go into their doctors’ offices with well-articulated complaints. The result is prescriptions.
Then, a significant percentage of patients simply do not fill their prescriptions. A significant percentage of the rest do not refill their prescriptions. And the drop-off continues. For the companies selling the drugs, these unfilled prescriptions look like lost sales. They are lost opportunities, and reduce the return on investment of all of the other interventions made to get prescriptions into the hands of patients. An ad for a podcast reads: ‘As regulatory hurdles mount and product pipelines shrivel, pharma companies must seek new revenue drivers to maintain growth. Addressing patient adherence, and thereby improving health outcomes and increasing potential revenue, is a popular answer to the problem.’33
The pharmaceutical industry is not alone in seeing ‘patient adherence’ (or ‘patient compliance’, though this term is falling out of favour because of its more obvious paternalism) as a huge problem. Drug distributors and pharmacies also see this problem in terms of lost sales: real customers are brought very close to their businesses, but then turn away at the last moment. And for many in the medical profession, non-adherence is dangerous and is contributing to the ill health of populations. If a physician writes a prescription, filling it should be in the patient’s best interests, all else being equal.
As a result, on display at industry conferences on patient adherence is a fascinating mix of idealism about patient outcomes, scientific interest in what leads people to take and not take medications, and cold calculation about returns on investment. For example, a single slide at a 2010 presentation displayed widely cited and widely repeated estimates that non-adherence is responsible for 125,000 deaths each year in the US and 11% of hospitalizations,34 a recognition of the complexity of the issue, and the claim that the US industry loses $30 billion annually to non-adherence. In the end, return on investment dominates, because in bold on the same slide is ‘Opportunity: A 3% increase in adherence translates to $1.0 billion in revenue for the pharmaceutical industry’.
Given the sales opportunities involved, many of the presenters at industry conferences on adherence are peddling something, usually in transparent ways. They represent firms offering products, services and expertise, and they want the pharmaceutical industry to pay for their programmes. Increased sales, they chime, will provide a healthy return on investment in these programmes.35
A Paradox?
For the pharmaceutical industry, one of the worst features of the patient non-adherence problem is that it seems intractable. Although measurements vary considerably – among researchers, among disease groups, among kinds of treatments – overall patient non-adherence is consistently and stubbornly high.
At industry conferences on patient adherence, a typical presenter might lead with some figures on the number of prescriptions filled and refilled. For example, Mr Allen, working for a firm that helps large organizations manage their health benefits, provides these numbers: 88% of prescriptions are filled, 76% are taken and 48% are refilled. Dr Anderson, who works for a large pharmaceutical company, asserts that, across many diseases, roughly 15% of prescriptions aren’t filled, and that of those that are, 28% are not refilled after thirty days, and 50% have stopped the treatment after six months. Mr Alvarez, an independent consultant, breaks down adherence rates by conditions. He reports that for treatment of type-2 diabetes, only 53% of patients are taking their medications after three months, 41% after six months, and 38% after twelve months. In Alvarez’s presentation, rates for many other conditions are similar, though depression is an outlier with only 30% of patients taking their medication after three months.
These estimates vary somewhat, and vary in how they are measured and reported. But more striking is just how similar they are. Moreover, Dr Anderson insists that the general picture hasn’t changed much during her long experience of working on the issue – though scientific understandings of the issue have changed considerably. Non-adherence seems to be a constant problem for the industry. Other research agrees: overviews and systematic reviews show reasonably consistent adherence levels over time.36
Yet many people at these conferences are presenting solutions to sell to pharma companies and other interested parties. Not only are they presenting solutions, but they appear to be presenting proven solutions, with data demonstrating that they really work. These solutions range widely. They include programmes in which pharmacists, nurses and others engage patients throughout the duration of their prescriptions; specialized agencies are happy to sell such services to pharmaceutical companies. There are phone apps that reward patients for checking in on their phones when they take their drugs. There are programmes to make refilling prescriptions easier – including having packages of drugs delivered directly to patients. There are devices to help patients and healthcare providers track whether and when drugs are being taken.
Ms Alexander, who works for a large pharma company, describes the analysis that led to a programme to focus on a particular group of patients prescribed a statin to reduce their cholesterol levels. To move the average number of ‘days on therapy’ for this group from 162 to 216, their costs for the drugs had to drop only slightly. The result was an increase in sales of $58 million, for a mere $3 million total wholesale price drop, or a return on investment of 18:1.
Another presenter, Mr Arnold, is transparently selling a product. His small device attaches to the top of a pill bottle, glows when it’s time to take a pill, chimes an hour after a pill has been missed, and transmits information via Wi-Fi whenever the pill bottle is opened. This allows monitors – perhaps paid for by the drug company and working in a call centre – to spot a missed day and call the patient. The cap will even contact an online pharmacy to deliver a refill of the prescription, with a simple push of a large button. According to Arnold’s company’s study, the system increases adherence by 27%.
How can we reconcile the persistence of non-adherence with the development and deployment of so many creative and effective interventions?
Almost certainly, effective drug marketing up to the point of prescription increases the challenge of non-adherence. In assemblage marketing, eventual demand is a product of initial demand and marketing effort. Without careful work to address patients themselves, marketing efforts can increase the costs and decrease the benefits as felt by some patients.
To explain this, let me take a very slight detour. In a provocative article, bioethicist Howard Brody and sociologist Donald Light argue that pharmaceutical marketing itself makes drugs less effective and less safe. They call the result the ‘inverse benefit law’: ‘The ratio of benefits to harms among patients taking new drugs tends to vary inversely with how extensively the drugs are marketed.’37 Their central argument is straightforward. Imagine that there is some ideal population of patients for some new drug, for all of whom the benefit-to-risk ratio is at the right level or higher, whatever the ‘right level’ is. Pharmaceutical marketing is aimed at increasing the patient population for drugs. But the benefit-to-risk ratio for the additional patients will be at a lower level than it was for the original ideal population, and so won’t be at the right level.
Brody and Light point out that many of the industry’s technical strategies feed directly into the inverse benefit law. For example, the industry attempts to expand patient populations by supporting research and guidelines that reduce thresholds for diagnoses of particular illnesses. Industry research also promotes studies that focus on surrogate markers and risk factors, rather than on the diseases that presumably sit behind them; there are far more cases of elevated cholesterol levels than of heart attacks.
To the extent that patients perceive that the balance among costs, risks and benefits isn’t worth it, they will tend to be non-adherent. There is no paradox, then. Programmes to reduce non-adherence work, but the industry’s very success at increasing prescriptions tends to increase non-adherence. The result is that non-adherence is a recalcitrant problem. Adherence programmes then become an additional part of assemblage marketing, and work in concert with everything else.
Shaping Patients’ Actions, Changing Patients’ Behaviour
Other than its apparent cost to the industry, patient non-adherence is a poorly understood problem. I was struck by how almost everybody at adherence conferences has a different approach to understanding the causes of the issue, leading to some divides when it comes to addressing it.
One senior figure in the field, Dr Anderson, is a commanding presence at one adherence conference. Everybody else seems deferential, and she is mentioned many times. A friendly-looking social scientist in her mid-sixties, Anderson has spent most of her career studying non-adherence and related phenomena, working within a large pharma company. She gives a presentation summarizing a history of changing models of non-adherence and what she takes to be the key take-home messages of the past generation of qualitative research on the topic. In particular, she claims, patients’ non-adherence is the result of a cost-benefit analysis involving concerns, benefits and needs; patients make active and reasoned decisions about filling prescriptions and taking their drugs. There is, then, no non-adherent personality (the focus of study of the phenomenon in the 1960s); nor are there non-adherent demographics.
Many of the speakers agree. They emphasize problems in communication, and how these can be remedied with the right interventions. Twenty-five percent of patients do not tell their physician if they stop taking a drug, reports Mr Armstrong, and physicians are poor at predicting which patients will become non-adherent. So, to pick just one of the facts that Armstrong lists, there are 33% more refills among patients who, when switched to a different cholesterol medication, are told why the new medication is the right one. Patients need to be given information in order to make a good decision.
Pharmacists can be particularly valuable, and many of the interventions are or involve programmes to pay pharmacists to spend more time with patients, both at the point of the original prescription, and again when the patients return for refills. Representatives of different pharmacy chains describe several nearly identical programmes. One speaker describes how pharmacists can be trained in ‘motivational interviewing’, which makes a two- to five-minute consultation session effective.
An article in an industry magazine touts new technologies as solving the problem of communication. It lists the following, almost all of them focused on communicating with patients to lead them to make more adherent decisions: ‘Smart phone apps that remind patients to take medication at the correct time; Websites to present disease and product information; Emails focused on product, disease or condition; Automated reminder calls; Surveys to engage patients and improve program; Text messaging focused on compliance; Call centre to handle inbound calls compliantly; Emails focused on compliance; Apps that [educate] and inform patients, their families and caretakers; Desktop reminder tools focused on compliance; RSS feeds focused on compliance; Calendar stickers focused on compliance’.38
Despite Dr Anderson’s emphasis on the rational patient, and notwithstanding the fact that she is treated as the most expert on the issue, a number of the other presenters at the same conference talk in terms of cause-and-effect models. They put forward remedies framed in terms of interventions that change patients’ behaviour, not their reasoning. For these speakers, good programmes address patients at least partly in terms of triggering preferred behaviour, rather than in terms of making rational decisions. A patient engagement manager at a large pharmaceutical company insists that ‘knowledge is not power’, and that because of this, her company has moved to ‘behavioural programmes’. Another speaker claims that there is no correlation between patient knowledge and adherence, and that ‘over a hundred studies’ prove it.
Although most of the presenters at these conferences work for pharma companies, pharma distributors, chains of pharmacies and specialized agencies, there are among them a few academic researchers. One group of university professors presents the results of a large quantitative meta-analysis of interventions to improve adherence in seniors. Their take-home message is that behavioural modifications are most likely to be successful: special packaging, dose modification, stimuli to take medications, and self-monitoring of some outcome such as blood pressure. Patient education, they argue, is generally not effective, unless it is in the form of succinct written instructions used as a prompt. On this issue, academic medicine and the pharmaceutical industry are having the same discussion.
Mr Allen makes one of a number of direct pitches for behaviourist approaches: ‘We have long used financial incentives … Now we’re finding that tools that build upon the insights of behavioural economics and psychology can have powerful, positive effects.’39 Allen builds a theoretical account of his programme, starting with three psychological bases: (1) ‘loss aversion’, the claim that in most situations people care more about losses than gains, (2) the ‘social norms’ principle that social comparisons drive consumer behaviour, and (3) the idea of ‘hyperbolic discounting’, that people value small, immediate rewards more than larger ones in the future. With this in the background, Allen claims that the messaging and other interventions in his programme were derived from these principles. It looks to me as though he is merely applying a gloss of science to his work, because the connections to the programme are somewhat opaque. Nonetheless, that gloss highlights the value of exploiting ways in which people don’t make decisions that are conventionally seen as rational. I have no reason to doubt that value.
Segmentation and Integration
Most of the work addressing non-adherence combines different approaches, modelling patients as making rational decisions but as influenced by other factors. For example, Mr Agnelli, CEO of an adherence-focused company, sets up a pairing between ‘behaviour modification’ – involving ‘classical conditioning, operant conditioning and social conditioning’ – and ‘pedagogical science’ – with its ‘integrative learning, experiential learning and timed learning’. The result, claims Agnelli, is a ‘comprehensive behavioural system’ on which the company builds a tailored programme with multiple, integrated channels. Again, I suspect that there is a certain amount of scientific gloss being applied to the programme, but it comes with good efficacy data from an RCT of patients with type-2 diabetes.
Since no one approach to addressing patient adherence is completely successful, programmes need to be focused on the right sub-segment. ‘Why don’t people adhere to their medicine regimens?’, asks Agnelli. ‘Each person has his or her own set of complex and interrelated reasons.’
To address these reasons, many people are mining databases. For one brand, a pair of presenters working for a big pharmaceutical company and a healthcare services company respectively set out an adherence goal of increasing ‘days on therapy’ by 10%. Their central pitch is about the importance of leveraging patient data to increase patient adherence. The key is to segment the patient population by building on surveys and databases. Some patients may respond better to a ‘co-pay card’ that gives them a discount on their portion of the drug costs. Some may respond better to an information campaign that reminds them about the benefits of staying on the drug and the risks of going off it. Some may respond well to face-to-face contact. Adherence experts develop playbooks for patients.
Even within communication approaches, segmentation of data is important. One speaker, Mr Adler, presents a European case study on ‘driving profitable behaviour through engagement’, where the drug in question is suboxone, a treatment for opioid addiction. For this drug, non-adherence rates are many times higher than for most other kinds of drugs. Adler divides the population into four categories, and then provides ‘key insights’ about the patient type, and ‘communication strategies’ and a ‘channel strategy’ for each. Figure 6.1 is a simplified version of the table he presents.
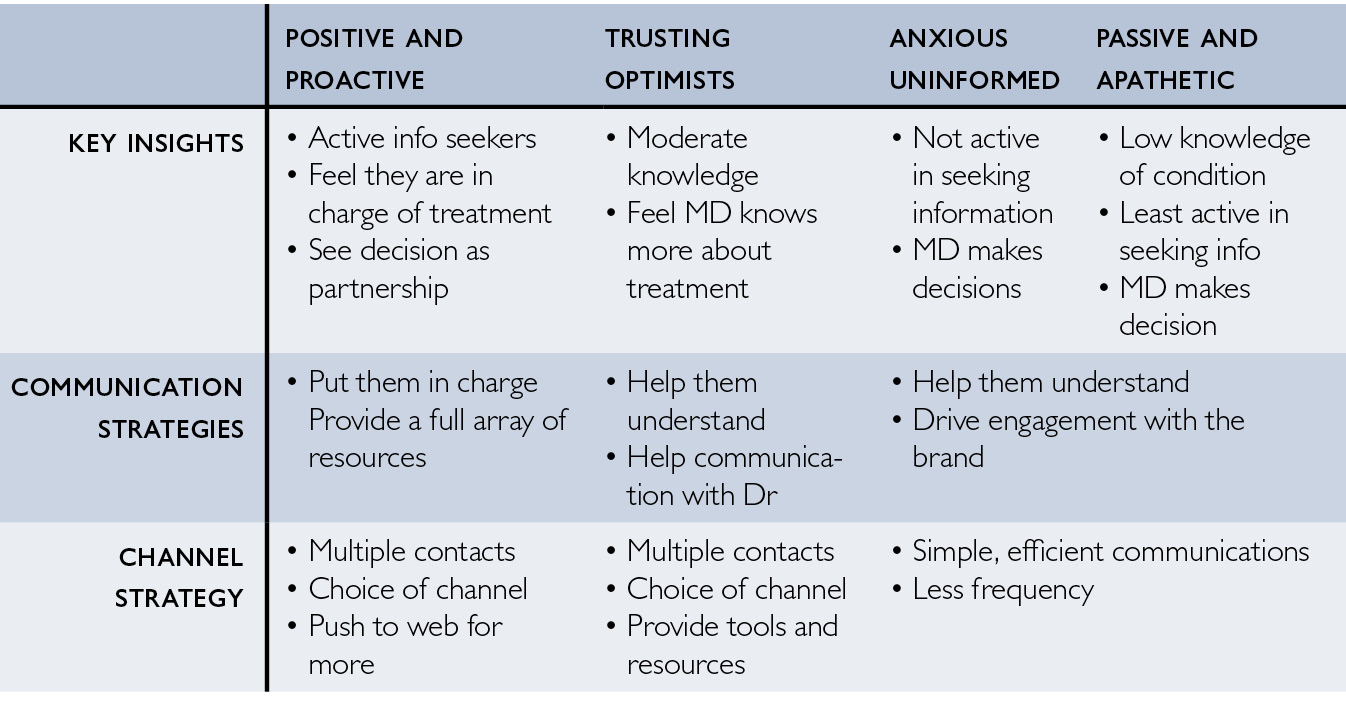
Fig. 6.1 Segmenting patient populations to improve adherence
Adler goes on to articulate these strategies in terms of media for communication, whether social media, SMS reminders, websites, or telephone contact. For each patient segment, the communication strategies are paired with differently timed cash payments, as incentives for engagement. But there remains the problem of how to measure the success of the programme. Patient adherence is tricky to measure, but in Adler’s case study a control group of patients were taking the drug but opted not to join the communication programme. For a modest cost of €55 per patient, the number of patients in the communication group was five times higher than the number in the control group.
A presenter working for a firm specializing in adherence programmes offers a stunningly comprehensive approach. Working with a sizeable number of pharmacy chains, the firm has developed a database covering nearly 50% of US patients, their addresses, and their pharmacy transactions going back many years – and often current to the previous week. The firm’s deluxe programme, presented through a case study of a blood pressure drug, includes five different components: (1) a letter-based campaign targeting patients at high risk of non-adherence, (2) an autofill programme by which patients will receive refills of their prescription delivered to their homes, (3) a face-to-face compliance programme involving initial counselling by pharmacists and follow-up phone monitoring, paid for by the drug company, (4) packaging that helps patients keep track of their medication consumption, and that advertises the compliance programme, and (5) a phone-based programme that follows up on prescriptions with direct-to-patient endorsement of the drug. The deluxe programme makes it very challenging for patients to casually stop taking the drug. The firm in question sponsored the wine and cheese reception at the conference.
Mr Alvarez presents several case studies on increasing ‘patient-centricity’, focusing most on a campaign to drive a particular statin use and adherence in Mexico. ‘Lack of adherence is often an emotional and conscious decision on the part of the patient to stop taking the medication [and] in such situations the traditional pharma-sponsored programmes sending out messages to remind patients to take their pill are going to be of limited effectiveness.’ He identifies opportunities for pharmaceutical companies to up their game, including ‘improving customer service’ and drawing on ‘patient advocacy’ and ‘peer-to-peer communication’. These are areas in which Alvarez’s company sees itself as particularly innovative, and he presents examples of magazines and websites owned by the company and used as vehicles to allow patient organizations to reach out to patients and help make them more adherent to treatments. In the Mexican campaign, his company built a database of patients, offering a 50% discount on the drugs for those who registered. This database became the infrastructure for establishing ongoing relationships with those patients. The campaign as a whole saw a 350% increase in sales of the drug.
Patient-centricity can bring together pharma companies and patient advocacy organizations (PAOs), the focus of the next chapter. In an interview, Mr Code, a very reflective marketing consultant in the UK, told me about a compliance project he had been involved in, to do with asthma patients not refilling or not renewing their prescriptions for inhalers. The company’s view was, ‘We don’t need more patients, we just need the blooming patients to be compliant!’ To that end, says Code, ‘we either created or we seeded [an] idea with the UK’s major patient advocacy group in asthma’. The idea was to fund trained nurses to ‘go into doctors’ surgeries … and put this proposition on the table that there were patients who were dying who shouldn’t be dying’. The nurses would then identify asthma patients who hadn’t been seen for a long time, and arrange for the clinic to contact them to encourage them to come in for a fresh evaluation, or perhaps just a renewal of their prescription. The company paid for the nurses for the first few years, though it routed those payments through the asthma PAO.
We should not forget the appeals to idealism. Even the most revenue-focused actors in the adherence world justify what they are doing in terms of helping patients. They see marketing and increasing patients’ welfare as entirely compatible. For this reason, across different adherence conferences, and in multiple talks, presenters quote former US Surgeon General C. Everett Koop: ‘Drugs don’t work in patients who don’t take them.’
‘Scripts’ and Scripts
Sales reps often refer to prescriptions as ‘scripts’. Although ‘script’ is merely an insider’s shorthand, the prescription is a script and is surrounded by scripts, in the ordinary sense. Prescriptions contain directions for pharmacists (the name, strength, quantity and number of refills of a drug to be sold to the patient) and for patients (the quantity of drugs to be consumed, and the frequency, duration and circumstances of consumption). But prescription may also be a result of sales reps’ many scripts for influencing doctors, and of doctors following the scripts that reps try to get them to adopt. Patients may then be following the scripts given to them by their doctors, among others, and may be helped to do so by the efforts of adherence specialists. All in all, pharma tries to shape the behaviours of physicians and patients, allowing them the appearance of agency while doing as much as possible to constrain it.